
.
2015, “A cluster randomised trial of cloth masks compared with medical masks in healthcare workers,” bmj.com. (Posted below)
……………………………………….
Added: Authors of 2015 study publish comment on March 30, 2020:
Authors of 2015 study, “the only published randomised controlled clinical trial of cloth masks,” comment in 2020 on issue of cloth masks and health care workers vs Covid:
- C Raina MacIntyre1,
- Holly Seale1,
- Tham Chi Dung2,
- Nguyen Tran Hien2,
- Phan Thi Nga2,
- Abrar Ahmad Chughtai1,
- Bayzidur Rahman1,
- Dominic E Dwyer3,
- Quanyi Wang4
“The authors of this article, published in 2015, have written a response to their work in light of the COVID-19 pandemic. We urge our readers to consider the response when reading the article. https://bmjopen.bmj.com/content/5/4/e006577.responses#covid-19-shortages-of-masks-and-the-use-of-cloth-masks-as-a-last-resort
………………..
Objective: The aim of this study was to compare the efficacy of cloth masks to medical masks in hospital healthcare workers (HCWs). The null hypothesis is that there is no difference between medical masks and cloth masks.
Setting 14 secondary-level/tertiary-level hospitals in Hanoi, Vietnam.
Participants 1607 hospital HCWs aged ≥18 years working full-time in selected high-risk wards.
Intervention Hospital wards were randomised to: medical masks, cloth masks or a control group (usual practice, which included mask wearing). Participants used the mask on every shift for 4 consecutive weeks.
Main outcome measure Clinical respiratory illness (CRI), influenza-like illness (ILI) and laboratory-confirmed respiratory virus infection.
Results The rates of all infection outcomes were highest in the cloth mask arm, with the rate of ILI [influenza like illness] statistically significantly higher in the cloth mask arm (relative risk (RR)=13.00, 95% CI 1.69 to 100.07) compared with the medical mask arm. Cloth masks also had significantly higher rates of ILI compared with the control arm. An analysis by mask use showed ILI (RR=6.64, 95% CI 1.45 to 28.65) and laboratory-confirmed virus (RR=1.72, 95% CI 1.01 to 2.94) were significantly higher in the cloth masks group compared with the medical masks group. Penetration of cloth masks by particles was almost 97% and medical masks 44%.
Conclusions This study is the first RCT of cloth masks, and the results caution against the use of cloth masks. This is an important finding to inform occupational health and safety. Moisture retention, reuse of cloth masks and poor filtration may result in increased risk of infection. Further research is needed to inform the widespread use of cloth masks globally. However, as a precautionary measure, cloth masks should not be recommended for HCWs, particularly in high-risk situations, and guidelines need to be updated.
Trial registration number Australian New Zealand Clinical Trials Registry: ACTRN12610000887077.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
*The use of cloth masks is widespread around the world, particularly in countries at high-risk for emerging infections, but there have been no efficacy studies to underpin their use.
*The use of cloth masks are not addressed in most guidelines for health care workers—this study provides data to update guidelines.
*The control arm was ‘standard practice’, which comprised mask use in a high proportion of participants. As such (without a no-mask control), the finding of a much higher rate of infection in the cloth mask arm could be interpreted as harm caused by cloth masks, efficacy of medical masks, or most likely a combination of both.
Introduction
The use of facemasks and respirators for the protection of healthcare workers (HCWs) has received renewed interest following the 2009 influenza pandemic,1 and emerging infectious diseases such as avian influenza,2 Middle East respiratory syndrome coronavirus (MERS-coronavirus)3,4 and Ebola virus.5 Historically, various types of cloth/cotton masks (referred to here after as ‘cloth masks’) have been used to protect HCWs.6 Disposable medical/surgical masks (referred to here after as ‘medical masks’) were introduced into healthcare in the mid 19th century, followed later by respirators.7 Compared with other parts of the world, the use of face masks is more prevalent in Asian countries, such as China and Vietnam.8–11
In high resource settings, disposable medical masks and respirators have long since replaced the use of cloth masks in hospitals. Yet cloth masks remain widely used globally, including in Asian countries, which have historically been affected by emerging infectious diseases, as well as in West Africa, in the context of shortages of personal protective equipment (PPE).12 ,13 It has been shown that medical research disproportionately favours diseases of wealthy countries, and there is a lack of research on the health needs of poorer countries.14 Further, there is a lack of high-quality studies around the use of facemasks and respirators in the healthcare setting, with only four randomised clinical trials (RCTs) to date.15 Despite widespread use, cloth masks are rarely mentioned in policy documents,16 and have never been tested for efficacy in a RCT. Very few studies have been conducted around the clinical effectiveness of cloth masks, and most available studies are observational or in vitro.6 Emerging infectious diseases are not constrained within geographical borders, so it is important for global disease control that use of cloth masks be underpinned by evidence. The aim of this study was to determine the efficacy of cloth masks compared with medical masks in HCWs working in high-risk hospital wards, against the prevention of respiratory infections.
Methods
A cluster-randomised trial of medical and cloth mask use for HCWs was conducted in 14 hospitals in Hanoi, Vietnam. The trial started on the 3 March 2011, with rolling recruitment undertaken between 3 March 2011 and 10 March 2011. Participants were followed during the same calendar time for 4 weeks of facemasks use and then one additional week for appearance of symptoms. An invitation letter was sent to 32 hospitals in Hanoi, of which 16 agreed to participate. One hospital did not meet the eligibility criteria; therefore, 74 wards in 15 hospitals were randomised. Following the randomisation process, one hospital withdrew from the study because of a nosocomial outbreak of rubella.
Participants provided written informed consent prior to initiation of the trial.
Randomisation
Seventy-four wards (emergency, infectious/respiratory disease, intensive care and paediatrics) were selected as high-risk settings for occupational exposure to respiratory infections. Cluster randomisation was used because the outcome of interest was respiratory infectious diseases, where prevention of one infection in an individual can prevent a chain of subsequent transmission in closed settings.8 ,9 Epi info V.6 was used to generate a randomisation allocation and 74 wards were randomly allocated to the interventions.
From the eligible wards 1868 HCWs were approached to participate. After providing informed consent, 1607 participants were randomised by ward to three arms: (1) medical masks at all times on their work shift; (2) cloth masks at all times on shift or (3) control arm (standard practice, which may or may not include mask use). Standard practice was used as control because the IRB deemed it unethical to ask participants to not wear a mask. We studied continuous mask use (defined as wearing masks all the time during a work shift, except while in the toilet or during tea or lunch breaks) because this reflects current practice in high-risk settings in Asia.8
The laboratory results were blinded and laboratory testing was conducted in a blinded fashion. As facemask use is a visible intervention, clinical end points could not be blinded. Figure 1 outlines the recruitment and randomisation process.

Figure 1
Consort diagram of recruitment and follow-up (HCWs, healthcare workers).
Primary end points
There were three primary end points for this study, used in our previous mask RCTs:8 ,9 (1) Clinical respiratory illness (CRI), defined as two or more respiratory symptoms or one respiratory symptom and a systemic symptom;17 (2) influenza-like illness (ILI), defined as fever ≥38°C plus one respiratory symptom and (3) laboratory-confirmed viral respiratory infection. Laboratory confirmation was by nucleic acid detection using multiplex reverse transcriptase PCR (RT-PCR) for 17 respiratory viruses: respiratory syncytial virus (RSV) A and B, human metapneumovirus (hMPV), influenza A (H3N2), (H1N1)pdm09, influenza B, parainfluenza viruses 1–4, influenza C, rhinoviruses, severe acute respiratory syndrome (SARS) associated coronavirus (SARS-CoV), coronaviruses 229E, NL63, OC43 and HKU1, adenoviruses and human bocavirus (hBoV).18–23 Additional end points included compliance with mask use, defined as using the mask during the shift for 70% or more of work shift hours.9 HCWs were categorised as ‘compliant’ if the average use was equal or more than 70% of the working time. HCW were categorised as ‘non-compliant’ if the average mask use was less than 70% of the working time.
Eligibility
Nurses or doctors aged ≥18 years working full-time were eligible. Exclusion criteria were: (1) Unable or refused to consent; (2) Beards, long moustaches or long facial hair stubble; (3) Current respiratory illness, rhinitis and/or allergy.
Intervention
Participants wore the mask on every shift for four consecutive weeks. Participants in the medical mask arm were supplied with two masks daily for each 8 h shift, while participants in the cloth mask arm were provided with five masks in total for the study duration, which they were asked to wash and rotate over the study period. They were asked to wash cloth masks with soap and water every day after finishing the shifts. Participants were supplied with written instructions on how to clean their cloth masks. Masks used in the study were locally manufactured medical (three layer, made of non-woven material) or cloth masks (two layer, made of cotton) commonly used in Vietnamese hospitals. The control group was asked to continue with their normal practices, which may or may not have included mask wearing. Mask wearing was measured and documented for all participants, including the control arm.
Data collection and follow-up
Data on sociodemographic, clinical and other potential confounding factors were collected at baseline. Participants were followed up daily for 4 weeks (active intervention period), and for an extra week of standard practice, in order to document incident infection after incubation. Participants received a thermometer (traditional glass and mercury) to measure their temperature daily and at symptom onset. Daily diary cards were provided to record number of hours worked and mask use, estimated number of patient contacts (with/without ILI) and number/type of aerosol-generating procedures (AGPs) conducted, such as suctioning of airways, sputum induction, endotracheal intubation and bronchoscopy. Participants in the cloth mask and control group (if they used cloth masks) were also asked to document the process used to clean their mask after use.
We also monitored compliance with mask use by a previously validated self-reporting mechanism.8 Participants were contacted daily to identify incident cases of respiratory infection. If participants were symptomatic, swabs of both tonsils and the posterior pharyngeal wall were collected on the day of reporting.
Sample collection and laboratory testing
Trained collectors used double rayon-tipped, plastic-shafted swabs to scratch tonsillar areas as well as the posterior pharyngeal wall of symptomatic participants. Testing was conducted using RT-PCR applying published methods.19–23 Viral RNA was extracted from each respiratory specimen using the Viral RNA Mini kit (Qiagen, Germany), following the manufacturer’s instructions. The RNA extraction step was controlled by amplification of a RNA house-keeping gene (amplify pGEM) using real-time RT-PCR. Only extracted samples with the house keeping gene detected by real-time RT-PCR were submitted for multiplex RT-PCR for viruses.
The reverse transcription and PCRs were performed in OneStep (Qiagen, Germany) to amplify viral target genes, and then in five multiplex RT-PCR: RSVA/B, influenza A/H3N2, A(H1N1) and B viruses, hMPV (reaction mix 1); parainfluenza viruses 1–4 (reaction mix 2); rhinoviruses, influenza C virus, SARS-CoV (reaction mix 3); coronaviruses OC43, 229E, NL63 and HKU1 (reaction mix 4); and adenoviruses and hBoV (reaction mix 5), using a method published by others.18 All samples with viruses detected by multiplex RT-PCR were confirmed by virus-specific mono nested or heminested PCR. Positive controls were prepared by in vitro transcription to control amplification efficacy and monitor for false negatives, and included in all runs (except for NL63 and HKU1). Each run always included two negatives to monitor amplification quality. Specimen processing, RNA extraction, PCR amplification and PCR product analyses were conducted in different rooms to avoid cross-contamination.19 ,20
Filtration testing
The filtration performance of the cloth and medical masks was tested according to the respiratory standard AS/NZS1716.24 The equipment used was a TSI 8110 Filter tester. To test the filtration performance, the filter is challenged by a known concentration of sodium chloride particles of a specified size range and at a defined flow rate. The particle concentration is measured before and after adding the filter material and the relative filtration efficiency is calculated. We examined the performance of cloth masks compared with the performance levels—P1, P2 (=N95) and P3, as used for assessment of all particulate filters for respiratory protection. The 3M 9320 N95 and 3M Vflex 9105 N95 were used to compare against the cloth and medical masks.
Sample size calculation
To obtain 80% power at two-sided 5% significance level for detecting a significant difference of attack rate between medical masks and cloth masks, and for a rate of infection of 13% for cloth mask wearers compared with 6% in medical mask wearers, we would need eight clusters per arm and 530 participants in each arm, and intracluster correlation coefficient (ICC) 0.027, obtained from our previous study.8 The design effect (deff) for this cluster randomisation trial was 1.65 (deff=1+(m−1)×ICC=1+(25−1)×0.027=1.65). As such, we aimed to recruit a sample size of 1600 participants from up to 15 hospitals.
Analysis
Descriptive statistics were compared among intervention and control arms. Primary end points were analysed by intention to treat. We compared the event rates for the primary outcomes across study arms and calculated p values from cluster-adjusted χ2 tests25 and ICC.25 ,26 We also estimated relative risk (RR) after adjusting for clustering using a log-binomial model under generalised estimating equation (GEE) framework.27 We checked for variables which were unequally distributed across arms, and conducted an adjusted analysis accordingly. We fitted a multivariable log-binomial model, using GEE to account for clustering by ward, to estimate RR after adjusting for potential confounders. In the initial model, we included all the variables that had p value less than 0.25 in the univariable analysis, along with the main exposure variable (randomisation arm). A backward elimination method was used to remove the variables that did not have any confounding effect.
As most participants in the control arm used a mask during the trial period, we carried out a post-hoc analysis comparing all participants who used only a medical mask (from the control arm and the medical mask arm) with all participants who used only a cloth mask (from the control arm and the cloth arm). For this analysis, controls who used both types of mask (n=245) or used N95 respirators (n=3) or did not use any masks (n=2) were excluded. We fitted a multivariable log-binomial model, to estimate RR after adjusting for potential confounders. As we pooled data of participants from all three arms and analysed by mask type, not trial arm, we did not adjust for clustering here. All statistical analyses were conducted using STATA V.12.28
Owing to a very high level of mask use in the control arm, we were unable to determine whether the differences between the medical and cloth mask arms were due to a protective effect of medical masks or a detrimental effect of cloth masks. To assist in interpreting the data, we compared rates of infection in the medical mask arm with rates observed in medical mask arms from two previous RCTs,8,9 in which no efficacy of medical masks could be demonstrated when compared with control or N95 respirators, recognising that seasonal and geographic variation in virus activity affects the rates of exposure (and hence rates of infection outcomes) among HCWs. This analysis was possible because the trial designs were similar and the same outcomes were measured in all three trials. The analysis was carried out to determine if the observed results were explained by a detrimental effect of cloth masks or a protective effect of medical masks.
Results
A total of 1607 HCWs were recruited into the study. The participation rate was 86% (1607/1868). The average number of participants per ward was 23 and the mean age was 36 years. On average, HCWs were in contact with 36 patients per day during the trial period (range 0–661 patients per day, median 20 patients per day). The distribution of demographic variables was generally similar between arms (table 1). Figure 2 shows the primary outcomes for each of the trial arms. The rates of CRI, ILI and laboratory-confirmed virus infections were lowest in the medical mask arm, followed by the control arm, and highest in the cloth mask arm.
Table 1
Demographic and other characteristics by arm of randomisation
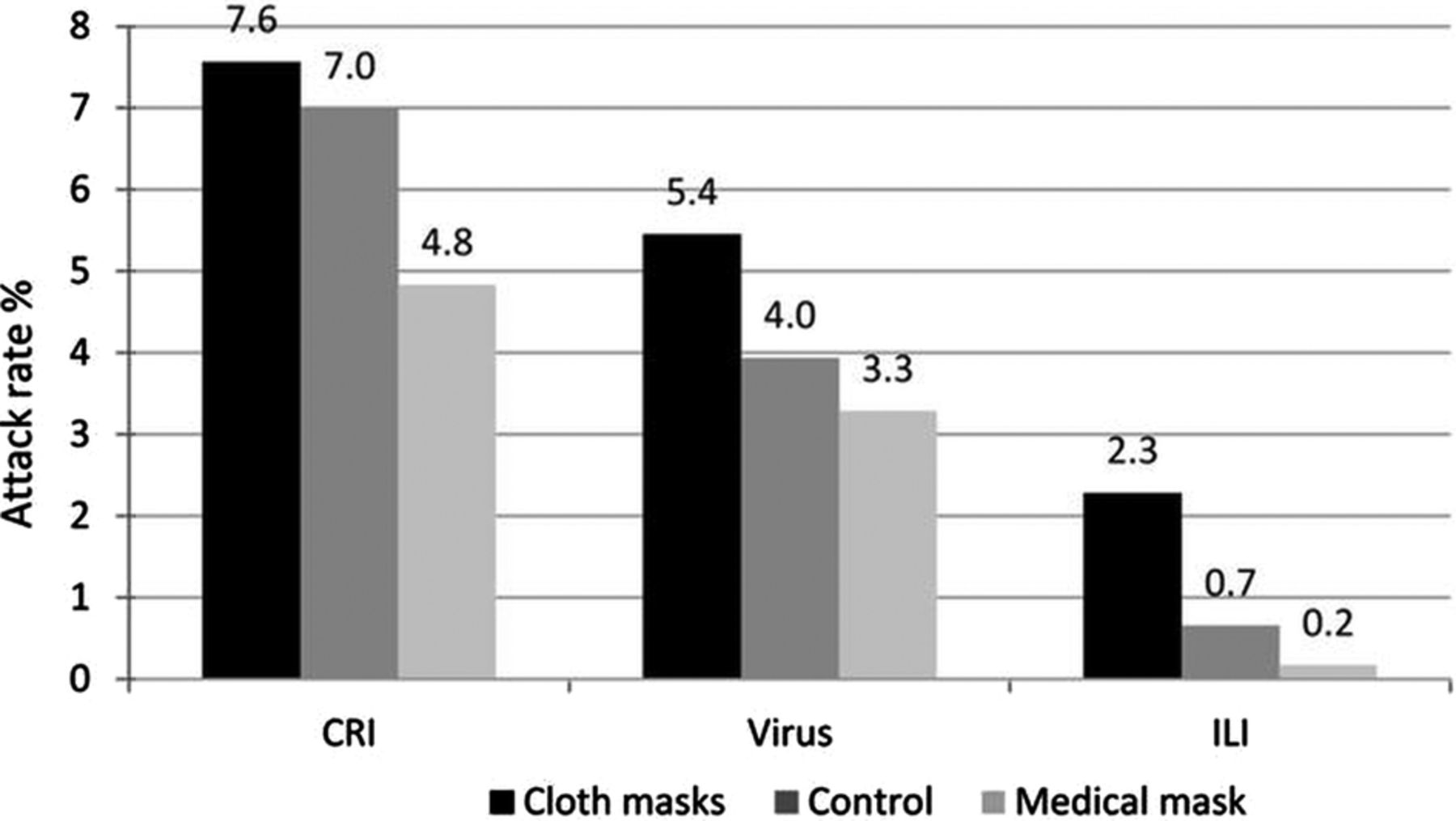
Figure 2
Outcomes in trial arms (CRI, clinical respiratory illness; ILI, influenza-like illness; Virus, laboratory-confirmed viruses).
Table 2 shows the intention-to-treat analysis. The rate of CRI was highest in the cloth mask arm, followed by the control arm, and lowest in the medical mask arm. The same trend was seen for ILI and laboratory tests confirmed viral infections. In intention-to-treat analysis, ILI was significantly higher among HCWs in the cloth masks group (RR=13.25 and 95% CI 1.74 to 100.97), compared with the medical masks group. The rate of ILI was also significantly higher in the cloth masks arm (RR=3.49 and 95% CI 1.00 to 12.17), compared with the control arm. Other outcomes were not statistically significant between the three arms.
Table 2
Intention-to-treat analysis
Among the 68 laboratory-confirmed cases, 58 (85%) were due to rhinoviruses. Other viruses detected were hMPV (7 cases), influenza B (1 case), hMPV/rhinovirus co-infection (1 case) and influenza B/rhinovirus co-infection (1 case) (table 3). No influenza A or RSV infections were detected.
Table 3
Type of virus isolated
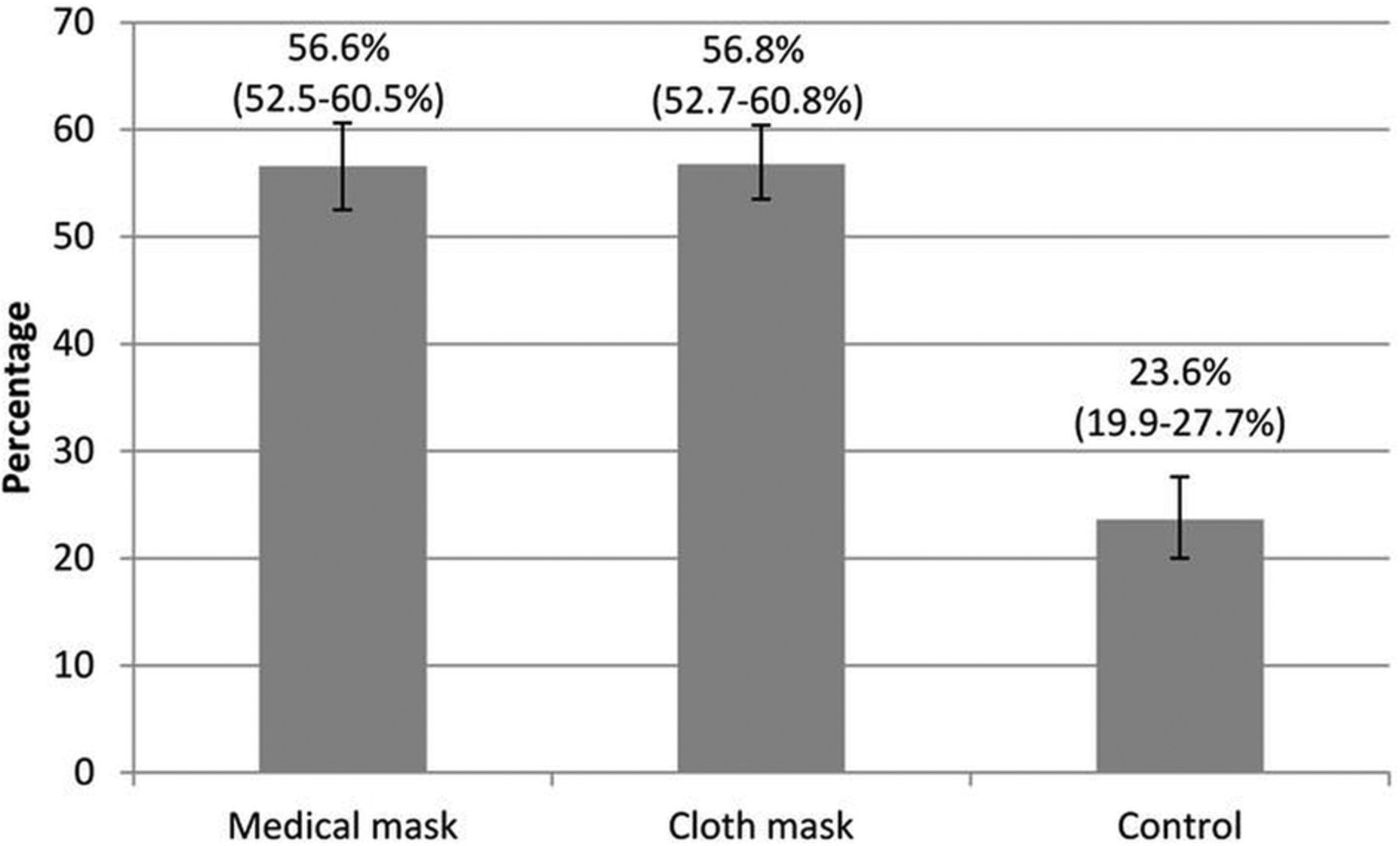
Compliance was significantly higher in the cloth mask arm (RR=2.41, 95% CI 2.01 to 2.88) and medical masks arm (RR=2.40, 95% CI 2.00 to 2.87), compared with the control arm. Figure 3 shows the percentage of participants who were compliant in the three arms. A post-hoc analysis adjusted for compliance and other potential confounders showed that the rate of ILI was significantly higher in the cloth mask arm (RR=13.00, 95% CI 1.69 to 100.07), compared with the medical masks arm (table 4). There was no significant difference between the medical mask and control arms. Hand washing was significantly protective against laboratory-confirmed viral infection (RR=0.66, 95% CI 0.44 to 0.97).
Table 4
Multivariable cluster-adjusted log-binomial model to calculate RR for study outcomes
{kind=link}
{kind=link}
{kind=link}
Figure 3
Compliance with the mask wearing—mask wearing more than 70% of working hours.
In the control arm, 170/458 (37%) used medical masks, 38/458 (8%) used cloth masks, and 245/458 (53%) used a combination of both medical and cloth masks during the study period. The remaining 1% either reported using a N95 respirator (n=3) or did not use any masks (n=2).
Table 5 shows an additional analysis comparing all participants who used only a medical mask (from the control arm and the medical mask arm) with all participants who used only a cloth mask (from the control arm and the cloth arm). In the univariate analysis, all outcomes were significantly higher in the cloth mask group, compared with the medical masks group. After adjusting for other factors, ILI (RR=6.64, 95% CI 1.45 to 28.65) and laboratory-confirmed virus (RR=1.72, 95% CI 1.01 to 2.94) remained significantly higher in the cloth masks group compared with the medical masks group.
Table 5
Univariate and adjusted analysis comparing participants who used medical masks and cloth masks*
Table 6 compares the outcomes in the medical mask arm with two previously published trials.8 ,9 This shows that while the rates of CRI were significantly higher in one of the previously published trials, the rates of laboratory-confirmed viruses were not significantly different between the three trials for medical mask use.
Table 6
A comparison of outcome data for the medical mask arm with medical mask outcomes in previously published RCTs
On average, HCWs worked for 25 days during the trial period and washed their cloth masks for 23/25 (92%) days. The most common approach to washing cloth masks was self-washing (456/569, 80%), followed by combined self-washing and hospital laundry (91/569, 16%), and only hospital laundry (22/569, 4%). Adverse events associated with facemask use were reported in 40.4% (227/562) of HCWs in the medical mask arm and 42.6% (242/568) in the cloth mask arm (p value 0.450). General discomfort (35.1%, 397/1130) and breathing problems(18.3%, 207/1130) were the most frequently reported adverse events.
Laboratory tests showed the penetration of particles through the cloth masks to be very high (97%) compared with medical masks (44%) (used in trial) and 3M 9320 N95 (<0.01%), 3M Vflex 9105 N95 (0.1%).
Discussion
We have provided the first clinical efficacy data of cloth masks, which suggest HCWs should not use cloth masks as protection against respiratory infection. Cloth masks resulted in significantly higher rates of infection than medical masks, and also performed worse than the control arm. The controls were HCWs who observed standard practice, which involved mask use in the majority, albeit with lower compliance than in the intervention arms. The control HCWs also used medical masks more often than cloth masks. When we analysed all mask-wearers including controls, the higher risk of cloth masks was seen for laboratory-confirmed respiratory viral infection.
The trend for all outcomes showed the lowest rates of infection in the medical mask group and the highest rates in the cloth mask arm. The study design does not allow us to determine whether medical masks had efficacy or whether cloth masks were detrimental to HCWs by causing an increase in infection risk. Either possibility, or a combination of both effects, could explain our results. It is also unknown whether the rates of infection observed in the cloth mask arm are the same or higher than in HCWs who do not wear a mask, as almost all participants in the control arm used a mask. The physical properties of a cloth mask, reuse, the frequency and effectiveness of cleaning, and increased moisture retention, may potentially increase the infection risk for HCWs. The virus may survive on the surface of the facemasks,29 and modelling studies have quantified the contamination levels of masks.30 Self-contamination through repeated use and improper doffing is possible. For example, a contaminated cloth mask may transfer pathogen from the mask to the bare hands of the wearer. We also showed that filtration was extremely poor (almost 0%) for the cloth masks. Observations during SARS suggested double-masking and other practices increased the risk of infection because of moisture, liquid diffusion and pathogen retention.31These effects may be associated with cloth masks.
We have previously shown that N95 respirators provide superior efficacy to medical masks,8 ,9 but need to be worn continuously in high-risk settings to protect HCWs.9 Although efficacy for medical masks was not shown, efficacy of a magnitude that was too small to be detected is possible.8 ,9 The magnitude of difference between cloth masks and medical masks in the current study, if explained by efficacy of medical masks alone, translates to an efficacy of 92% against ILI, which is possible, but not consistent with the lack of efficacy in the two previous RCTs.8 ,9 Further, we found no significant difference in rates of virus isolation in medical mask users between the three trials, suggesting that the results of this study could be interpreted as partly being explained by a detrimental effect of cloth masks. This is further supported by the fact that the rate of virus isolation in the no-mask control group in the first Chinese RCT was 3.1%, which was not significantly different to the rates of virus isolation in the medical mask arms in any of the three trials including this one. Unlike the previous RCTs, circulating influenza and RSV were almost completely absent during this study, with rhinoviruses comprising 85% of isolated pathogens, which means the measured efficacy is against a different range of circulating respiratory pathogens. Influenza and RSV predominantly transmit through droplet and contact routes, while Rhinovirus transmits through multiple routes, including airborne and droplet routes.32,33 The data also show that the clinical case definition of ILI is non-specific, and captures a range of pathogens other than influenza. The study suggests medical masks may be protective, but the magnitude of difference raises the possibility that cloth masks cause an increase in infection risk in HCWs. Further, the filtration of the medical mask used in this trial was poor, making extremely high efficacy of medical masks unlikely, particularly given the predominant pathogen was rhinovirus, which spreads by the airborne route. Given the obligations to HCW occupational health and safety, it is important to consider the potential risk of using cloth masks.
In many parts of the world, cloth masks and medical masks may be the only options available for HCWs. Cloth masks have been used in West Africa during the Ebola outbreak in 2014, due to shortages of PPE, (personal communication, M Jalloh). The use of cloth masks is recommended by some health organisations, with caveats.34–36 In light of our study, and the obligation to ensure occupational health and safety of HCWs, cloth masks should not be recommended for HCWs, particularly during AGPs and in high-risk settings such as emergency, infectious/respiratory disease and intensive care wards. Infection control guidelines need to acknowledge the widespread real-world practice of cloth masks and should comprehensively address their use. In addition, other important infection control measure such as hand hygiene should not be compromised. We confirmed the protective effects of hand hygiene against laboratory-confirmed viral infection in this study, but mask type was an independent predictor of clinical illness, even adjusted for hand hygiene.
A limitation of this study is that we did not measure compliance with hand hygiene, and the results reflect self-reported compliance, which may be subject to recall or other types of bias. Another limitation of this study is the lack of a no-mask control group [due to ethical concerns] and the high use of masks in the controls, which makes interpretation of the results more difficult. In addition, the quality of paper and cloth masks varies widely around the world, so the results may not be generalisable to all settings. The lack of influenza and RSV (or asymptomatic infections) during the study is also a limitation, although the predominance of rhinovirus is informative about pathogens transmitted by the droplet and airborne routes in this setting. As in previous studies, exposure to infection outside the workplace could not be estimated, but we would assume it to be equally distributed between trial arms. The major strength of the randomised trial study design is in ensuring equal distribution of confounders and effect modifiers (such as exposure outside the workplace) between trial arms.
Cloth masks are used in resource-poor settings because of the reduced cost of a reusable option. Various types of cloth masks (made of cotton, gauze and other fibres) have been tested in vitro in the past and show lower filtration capacity compared with disposable masks.7 The protection afforded by gauze masks increases with the fineness of the cloth and the number of layers,37 indicating potential to develop a more effective cloth mask, for example, with finer weave, more layers and a better fit.
Cloth masks are generally retained long term and reused multiple times, with a variety of cleaning methods and widely different intervals of cleaning.34 Further studies are required to determine if variations in frequency and type of cleaning affect the efficacy of cloth masks.
Pandemics and emerging infections are more likely to arise in low-income or middle-income settings than in wealthy countries. In the interests of global public health, adequate attention should be paid to cloth mask use in such settings. The data from this study provide some reassurance about medical masks, and are the first data to show potential clinical efficacy of medical masks. Medical masks are used to provide protection against droplet spread, splash and spray of blood and body fluids. Medical masks or respirators are recommended by different organisations to prevent transmission of Ebola virus, yet shortages of PPE may result in HCWs being forced to use cloth masks.38–40 In the interest of providing safe, low-cost options in low income countries, there is scope for research into more effectively designed cloth masks, but until such research is carried out, cloth masks should not be recommended. We also recommend that infection control guidelines be updated about cloth mask use to protect the occupational health and safety of HCWs.
Acknowledgments
The authors would like to thank the staff members from the National Institute of Hygiene and Epidemiology, Hanoi, Vietnam, who were involved with the trial. They thank as well to the staff from the Hanoi hospitals who participated. They also acknowledge the support of 3M for testing of filtration of the facemasks. 3M was industry partner in the ARC linkage project grant; however they were not involved in study design, data collection or analysis. The 3M products were not used in this study.
References
Footnotes
-
Contributors CRM was the lead investigator, and responsible for the conception and design of the trial, obtaining the grant funding, overseeing the whole study, analysing the data and writing of the report. HS contributed to overseeing the study, staff training, form/database development and drafting of the manuscript. TCD was responsible for overseeing the study, database management, recruitment, training and revision of the manuscript. NTH was responsible for the implementation of research and revision of the manuscript. PTN was responsible for the laboratory testing in Vietnam. AAC contributed to the statistical analysis and drafting of the manuscript. BR was responsible for the statistical analysis and revision of the manuscript. DED contributed to the laboratory technical assistance and revision of the manuscript. QW assisted in comparing the rates of infection from two previous RCTs conducted in China and revision of the manuscript.
-
Funding Funding to conduct this study was received from the Australian Research Council (ARC) (grant number LP0990749).
-
Competing interests CRM has held an Australian Research Council Linkage Grant with 3M as the industry partner, for investigator-driven research. 3M has also contributed masks and respirators for investigator-driven clinical trials. CRM has received research grants and laboratory testing as in-kind support from Pfizer, GSK and Bio-CSL for investigator-driven research. HS had a NHMRC Australian-based Public Health Training Fellowship at the time of the study (1012631). She has also received funding from vaccine manufacturers GSK, bio-CSL and Sanofi Pasteur for investigator-driven research and presentations. AAC used filtration testing of masks for his PhD thesis conducted by 3M Australia.
-
Ethics approval National Institute for Hygiene and Epidemiology (NIHE) (approval number 05 IRB) and the Human Research Ethics Committee of the University of New South Wales (UNSW), Australia, (HREC approval number 10306).
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.
Request Permissions
If you wish to reuse any or all of this article please use the link below which will take you to the Copyright Clearance Center’s RightsLink service. You will be able to get a quick price and instant permission to reuse the content in many different ways.
Chandini R MacIntyre, Academic physician The Kirby Institute, University of New South Wales. Other Contributors: Chi Dung Tham, Academic physician, Holly Seale, Academic, Abrar Chughtai, Academic physician
“Critical shortages of personal protective equipment (PPE) have resulted in the US Centers for Disease Control downgrading their recommendations for health workers treating COVID-19 patients from respirators to surgical masks and finally to home-made cloth masks. As authors of the only published randomised controlled clinical trial of cloth masks, we have been getting daily emails about this from health workers concerned about using cloth masks.The [2015] study [of 17 respiratory viruses] found that cloth mask wearers had higher rates of infection than even the standard practice control group of health workers, and the filtration provided by cloth masks was poor compared to surgical masks. At the time of the study, there had been very little work done in this space, and so little thought into how to improve the protective value of the cloth masks. Until now, most guidelines on PPE did not even mention cloth masks, despite many health workers in Asia using them.
Health workers are asking us if they should wear no mask at all if cloth masks are the only option. Our research does not condone health workers working unprotected.We recommend that health workers should not work during the COVID-19 pandemic without respiratory protection as a matter of work health and safety.In addition, if health workers get infected, high rates of staff absenteeism from illness may also affect health system capacity to respond. Some health workers may still choose to work in inadequate PPE. In this case, the physical barrier provided by a cloth mask may afford some protection, but likely much less than a surgical mask or a respirator.
It is important to note that some subjects in the control arm wore surgical masks, which could explain why cloth masks performed poorly compared to the control group. We also did an analysis of all mask wearers, and the higher infection rate in cloth mask group persisted. The cloth masks may have been worse in our study because they were not washed well enough – they may become damp and contaminated. The cloth masks used in our study were products manufactured locally, and fabrics can vary in quality. This and other limitations were also discussed.
There are now numerous reports of health workers wearing home made cloth masks, or re-using disposable mask and respirators, and asking for guidance. If health workers choose to work in these circumstances, guidance should be given around the use.
There have been a number of laboratory studies looking at the effectiveness of different types of cloth materials, single versus multiple layers and about the role that filters can play. However, none have been tested in a clinical trial for efficacy. If health workers choose to work using cloth masks, we suggest that they have at least two and cycle them, so that each one can be washed and dried after daily use. Sanitizer spray or UV disinfection boxes can be used to clean them during breaks in a single day. These are pragmatic, rather than evidence-based suggestions, given the situation.
Finally for COVID-19, wearing a mask is not enough to protect healthcare workers– use of gloves and goggles are also required as a minimum, as SARS-CoV-2 may infect not only through the respiratory route, but also through contact with contaminated surfaces and self-contamination.
Governments and hospitals should plan and stockpile proper disposable products such as respirators and surgical masks to ensure the occupational health and safety of health workers. This appears to have been a failure in many countries, including high income countries.”
We were the authors of the 2015 RCT [Randomized Controlled Trial], which was funded by an Australian Research Council Linkage Grant with 3M as the partner on the grant.”
When 85% of the viruses found in laboratory tests were rhinoviruses, which are about four times smaller than SARS-CoV2, no conclusion from this article can be applied to COVID-19/SARS-CoV2. No coronaviruses of any kind were found even though the tests were performed. Finally, their claim that “Penetration of cloth masks by particles was almost 97%” is of no value when the particles sizes are not stated. Furthermore, since many viruses, such as influenza, herpes simplex, and coronaviruses are surrounded by a fatty layer, called a “lipid envelope,” one wonders about the choice of sodium chloride particles instead of oil particles, taking in consideration that the instrument used (TSI 8110 Filter tester) can use either.”