After the "expert" computer model hustle, do we get our $2 trillion back? New York and US virus problems nearly vanish, just weeks ago NY begged feds for more ventilators for virus patients. Now it’s shipping ventilators to other states-Washington Times
“If their rate of spread actually happened, we would [have] been in a
much, much worse situation,” he said. “We slowed the infection by our
actions and that’s why we’re in a better position today.”
Total deaths, which had been projected to reach nearly 82,000 by August, are now projected at fewer than 70,000 in IHME’s latest data, which assumes full social distancing measures will last through May.
The national stockpile, which was down to about 6,900 ventilators on
Sunday, was back up to more than 8,700 on Wednesday, according to FEMA
numbers.
Dr. Anand Parekh, a former deputy assistant secretary at the U.S. Health Department and now chief medical advisor at the Bipartisan Policy Center, said the drop in demand for ventilators is likely due [meaning he’s guessing, not stating published peer reviewed results] to social distancing managing to flatten the curve, reducing the peak need for intensive care and medical equipment….
Just as people struggle with how to act in a forecast with a 40% chance of rain, so policymakers are making major decisions while grappling with large confidence intervals,
based on the factors Dr. Pham identified. [Not a problem. Simply cancel
the “major decision” to steal $2.2 trillion of “the folks” money].
“Models always include uncertainty and can never predict the exact numbers, and models are also changing with circumstances,” Mr. Ophir said. [Fine, so just return the $2.2 trillion of our money].
[Ed. note: You just said we “folks” were too stupid to understand “limits of the data,“now you say we should believe “models” suggesting “echo boom?” Of course, trillions more will be needed for that “suggestion.”]
(continuing): “social distancing is relaxed too far or too fast, and if a strong testing, tracking and isolation regime isn’t in place.
Dr. Parekh said [failed, so-called]policymakers [who’ve predicted the exact opposite so far and haven’t offered to return the $2.2 trillion it stole from the “folks”]need to plan for a rebound of cases.
“I think it’s critical that we continue the manufacturing and stockpiling of ventilators given that this is still the [alleged] first wave of the pandemic and we don’t quite know what [if anything] might come next,”he said.” ……………………………………….. Among comments: ………………………………………
“When Boris Johnson was campaigning for Britain to leave the European Union in 2016 — a path that many experts warned would end in disaster for the country — one of his close allies, Michael Gove, famously declared that “people in this country have had enough of experts.”
Now, Mr. Gove and Mr. Johnson are leading the British government as it confronts the calamity of the coronavirus, and Mr. Johnson, now the prime minister, insists the process is being guided by experts.The trouble is, those experts can often disagree with each other or change their minds about the right course of action.
“A lot of it is not what they say, but who says it,” said Devi Sridhar, director of the global health governance program at Edinburgh University. “Neil Ferguson has a huge amount of influence.”
Imperial College, experts noted, was part of the advisory group for the government’s now-abandoned strategy, which played down radical social distancing and accepted that the infection would spread through the population. The theory is that this would build up so-called “herd immunity,” so that the public would be more resistant in the face of a second wave of infections next winter.
But such a strategy, the report noted, would lead to a flood of critically ill patients in a country without enough beds. Instead, it said, Britain needs to pursue “suppression,” which involves far stricter lockdowns, like the closing of schools and the quarantine of infected people and their families. That would drive down the number of cases and spread out the flow of patients over a longer period, allowing hospitals to cope.
Dr. Ferguson has been candid that the report reached new conclusions because of the latest data from Italy,
which has seen a spiraling rate of infections, swamping hospitals and
forcing doctors to make agonizing decisions about who to treat.
But other experts said the burden on hospitals was clear as far back as the original outbreak in Wuhan, China. Lancet, the British medical journal, published an article in January, based on studying a small group of patients, which found that a third of people had to be admitted to intensive care units.
“We’re all using the 1918 pandemic flu handbook,” Dr. Sridhar said. “But we’re in a different position than in 1918. We’re in 2020.”
After days of confusion about the wisdom of encouraging “herd immunity,”
the government sought to play down the dispute, arguing that this was
not a deliberate part of its strategy but a byproduct of it. But it shifted to a policy of urging people not to go to pubs, restaurants, theaters or museums.
On Tuesday, the [UK] government’s chief scientific adviser, Sir Patrick Vallance, said he expected these new, more stringent restrictionsto last for months— and that the authorities would have to monitor very carefully what would happen when they are eventually lifted.
British officials recognize that their health service faces a moment of truth. All non-urgent operations in England will be postponed for at least three months, starting April 15, to free up 30,000 beds to help tackle the coronavirus.
Britain lags behind other European nations in its supply of ventilators.
Plans are underway to ramp up their numbers from over 8,000 to 12,000,
though officials are reluctant to promise that even this is sufficient.
Underscoring the change in tone, Britain’s finance chief, Rishi Sunak, announced a gargantuan fiscal stimulusto salvage reeling British businesses and to try to stem job losses. The
package, worth £330 billion, or $422 billion, will include
government-backed loans and tax breaks for companies and a three-month
break in mortgage repayments for strapped homeowners.
Professor Neil Ferguson, head of the MRC GIDA team and director of the Abdul Latif Jameel Institute for Disease and Emergency Analytics (J-IDEA), said: “The world is facing the most serious public health crisis in generations. Here we provide concrete estimates of the scale of the threat countries now face.
“We use the latest estimates of severity to show that policy strategies which aim to mitigate the epidemic might halve deaths and reduce peak healthcare demand by two-thirds, but that this will not be enough to prevent health systems being overwhelmed.
More intensive, and socially disruptive interventions will therefore be required to suppress transmission to low levels. It is likely such measures – most notably, large scale social distancing – will need to be in place for many months, perhaps until a vaccine becomes available [of course there’s no guarantee that a suitable vaccine will ever “become available”].”
Combining multiple measures
In the current absence of vaccines and effective drug treatments [with the exception of hydroxyquinalone cocktails which continue to show success], there are several public health measures countries can take to help slow the spread of the COVID-19. The team focused on the impact of five such measures, alone and in combination:
*Home isolation of cases – whereby those with symptoms of the disease (cough and/or fever) remain at home for 7 days following the onset of symptoms*Home quarantine – whereby all household members of those
with symptoms of the disease remain at home for 14 days following the
onset of symptoms
*Social distancing – a broad policy that aims to reduce overall contacts that people make outside the household, school or workplace by three-quarters. *Social distancing of those over 70 years – as for social
distancing but just for those over 70 years of age who are at highest
risk of severe disease *Closure of schools and universities
Modelling available data, the team found that depending on the intensity of the interventions, combinations would result in one of two scenarios.
In the first scenario, they show that interventions could slow down the spread of the infection but would not completely interrupt its spread. They found this would reduce the demand on the healthcare system while protecting those most at risk of severe disease. Such epidemics are predicted to peak over a three to four-month period during the spring/summer.
In the second scenario, more intensive interventions could interrupt transmission and reduce case numbers to low levels.
However, once these interventions are relaxed, case numbers are predicted to rise. This gives rise to lower case numbers, but the risk of a later epidemic in the winter months unless the interventions can be sustained. ........... .........
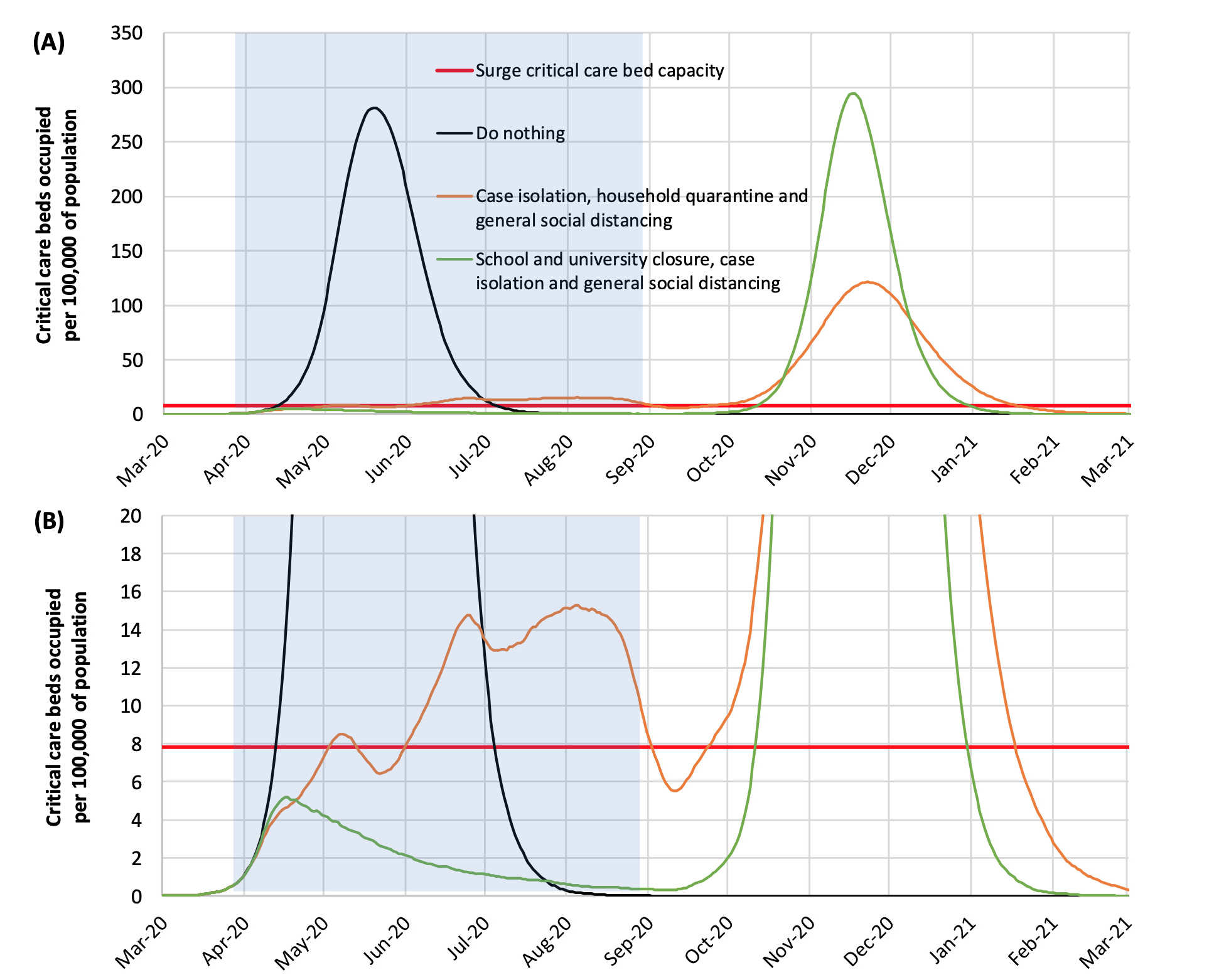
Flattening the curve: The report highlights suppression strategy scenarios for the UK showing intensive care unit (ICU) bed requirements. The black line shows the unmitigated epidemic. Green shows a suppression strategy incorporating closure of schools and universities, case isolation and population-wide social distancing beginning in late March 2020. The orange line shows a containment strategy incorporating case isolation, household quarantine and population-wide social distancing. The red line is the estimated surge ICU bed capacity in GB.
The blue shading shows the 5-month period in which these interventions
are assumed to remain in place. (B) shows the same data as in panel (A)
but zoomed in on the lower levels of the graph. (Source: WHO collaborating Centre / MRC GIDA / J-IDEA)Slowing and suppressing the outbreak
The report details that for the first scenario (slowing the spread), the optimal policy would combine home isolation of cases, home quarantine and social distancing of those over 70 years. This could reduce the peak healthcare demand by two-thirds and reduce deaths by half. However, the resulting epidemic would still likely result in an estimated 250,000 deaths and therefore overwhelm the health system (most notably intensive care units).
In the second scenario (suppressing the outbreak), the researchers show this is likely to require a combination of social distancing of the entire population, home
isolation of cases and household quarantine of their family members
(and possible school and university closure). The researchers explain
that by closely monitoring disease trends it may be possible for
these measures to be relaxed temporarily as things progress, but they
will need to be rapidly re-introduced if/when case numbers rise. They add that the situation in China and South Korea in the coming weeks will help to inform this strategy further.
Professor Azra Ghani,
Chair in Infectious Disease Epidemiology from the MRC Centre for Global
Infectious Disease Analysis, said: “The current situation with the
COVID-19 pandemic is evolving rapidly; governments and societies
therefore need to be flexible in responding the challenges it poses. Our results indicate that widescale social distancing measures,
that are likely to have a major impact on our day-to-day lives, are now
necessary to reduce further spread and prevent our health system being
overwhelmed. Close monitoring will be required in the coming weeks and
months to ensure that we minimise the health impact of this disease.”
Professor Christl Donnelly,
Professor of Statistical Epidemiology within J-IDEA, said: “The
challenges we collectively face are daunting. However, our work
indicates if a combination of measures are implemented, then
transmission can be substantially reduced. These measures will be
disruptive but uncertainties will reduce over time, and while we await effective vaccines [which may never exist] and drugs, these public health measures can reduce demands on our healthcare systems.”
Professor Steven Riley, Professor of Infectious Disease Dynamics within J-IDEA, said: “We have to accept that COVID-19 is a severe infection and it is currently able to spread in countries such as the US and the UK. In this report, we show that the most stringent traditional interventions are required
in the short term to halt its spread. Once they are in place, it
becomes a common priority for us all to find the best possible ways to
improve on those interventions”
The Imperial College COVID-19 Response Fund will
supplement government and existing philanthropy to provide flexible
support for vital projects in the university’s unprecedented efforts to
tackle COVID-19 such as developing vaccines, improving diagnostics,
advancing therapies, strengthening epidemiology and providing essential
healthcare in the urgent race to defeat the novel coronavirus.”

 .........
.........
No comments:
Post a Comment