.
Includes follow up to Dr. Fareed’s Nov. 19, 2020 U.S. Senate hearing, “Early Outpatient Treatment: An Essential Part of a Covid-19 Solution:”
12/12/20, “Dr. George Fareed and Dr. Brian Tyson share early treatment protocol,” The Desert Review, Brawley, Imperial Valley, Calif.
 “Dr. George Fareed, Imperial Valley [Calif.] frontline doctor fighting against the COVID-19 pandemic locally, has been fielding phone calls from across the nation helping those afflicted but unable to get early treatment from their medical establishments.
“Dr. George Fareed, Imperial Valley [Calif.] frontline doctor fighting against the COVID-19 pandemic locally, has been fielding phone calls from across the nation helping those afflicted but unable to get early treatment from their medical establishments.
“I’m really busy, but I’m willing to help anyone,” Fareed said.
The doctor reached out to The Desert Review suggesting publication of the Protocol he and Dr. Brian Tyson have refined for their local patients that has been so successful. Fareed also included in his material what Dr. Zelenko, a pioneer in repurposing medicines for the virus has developed as a prophylaxis, a preventative subscription [which is mainly zinc, Vitamin C, and Quercetin, posted below]….
[10/19/20, Dr. Brian Tyson reported 100% success rate treating Covid early.““We were at the heart of the pandemic due to our large Hispanic and diabetic population.” Dr. Tyson said Imperial Valley shares an international border in the south with Mexicali, Mexico which has a population of 1.5 million residents. He treated 1,900 positive patients….“We treated this virus early….We only had one hospitalization and zero deaths. Zero deaths, because we were not going to stand by and allow people to die without treatment,” Dr. Tyson said.” 10/19/20]
(continuing): “Also included in the material submitted, is a follow up to Dr. Fareed’s U.S. Senate hearing, “Early Outpatient Treatment: An Essential Part of a COVID-19 Solution” held November 19 in the Capitol.
 Senator Josh Hawley submitted questions to Dr. Fareed to clarify his testimony for the record. Here is the correspondence between the Senator and Fareed on December 10:
Senator Josh Hawley submitted questions to Dr. Fareed to clarify his testimony for the record. Here is the correspondence between the Senator and Fareed on December 10:
Sen. Hawley: In your testimony, you say that timing is everything when it comes to treatment and that the best time for outpatient treatment to prevent hospitalization comes when “the virus is in a period of maximum replication in the upper respiratory tract.” Can you explain what this would mean for a patient? Would this be five days after exposure, or ten days? Or is it based on symptoms?
Dr. Fareed: The earlier the treatment can be started after the start of the infection, the better and more rapid the recovery (as well as the reduction in the risk of spread/contagious period). This would mean that the patient should optimally start the treatment in the first 4 days of the infection and within five days of exposure. It usually is based on symptoms which start within 1-4 days of viral entry into the upper respiratory system. Even starting the multi-faceted treatment later (7-10 days after infection) is also very worthwhile if severe pneumonia necessitating hospitalization has not yet set in.
Sen. Hawley: In your experience, are patients typically coming in to get treated at this point in their illness? And if not, what do you think we need to do to encourage high-risk individuals to to seek outpatient treatment and care?
Dr. Fareed: More patients are coming in to get treated or contacting me from afar for treatment when they can’t receive the treatment in their local communities. Sadly, many infected people and primary care doctors and doctors in ERs follow the NIH and Dr. Fauci stipulations with no effective treatments offered. We need to have the NIH/FDA/CDC formally acknowledge the importance of early treatment with moderately acting, safe anti-virals so readily available. When (if ever) that happens, everything would improve dramatically. Thank you, Senator Hawley, for all your efforts and for allowing me to respond to these excellent questions.
The following is the protocol Drs. Fareed and Tyson have jointly developed as most effective for their COVID-19 patients:
Fareed/Tyson COVID-19 Treatment Protocol
HCQ 200 mg tabs [pills] #16 (HCQ = hydroxychloroquine) [HCQ was approved by FDA in 1955 and had been used in hundreds of millions of prescriptions worldwide since then. (scroll down)]
Zinc sulfate 22O mg (or elemental Zinc 50 mg) # 15
Azithromycin 500 mg # 5 (or Z pack) or
Doxycycline 100 mg # 10)
Ivermectin 3 mg tabs #8
Aspirin 325 mg tabs #30
Day 1 – HCQ 2 tabs twice a day
Zinc sulfate tab twice a day
(Azithromycin tab one per day or doxycycline cap twice a day)
Ivermectin 12 mg on day 1 only
Aspirin 325 mg
Days 2-5
HCQ tab 3 times a day
Zinc sulfate 3 times a day
(Azithromycin tab daily or doxycycline cap twice a day)
Aspirin 325 mg daily
Ivermectin 12 mg on day 3 if symptoms warrant
Prednisone 60 mg daily x 5-7 days or
Dexamethasone 4 mg bid if wheezing /SOB
Budesonide 0.5-1mg/2ml vía nebulizer bid
Vitamin D3 5000 iu daily
Pepcid 20 mg daily
Continue daily Aspirin 325 mg
Over the counter prevention:
Elemental Zinc 25 mg once a day
Vitamin D 4000 iu once a day
Vitamin C 1000 mg once a day
Quercetin 500 mg once a day
If Quercetin is unavailable, then use Epigallocatechin-gallate (EGCG) 400mg once a day
Dr. Fareed also included Dr. Zelenko’s (Twitter: @zev_dr [Here’s an alternate source for Dr. Zelenko’s work. On Dec. 23 twitter suspended Dr. Zelenko’s account.…Another helpful twitter site: https://twitter.com/CovidAnalysis]) COVID-19 Prophylaxis Protocol:
Prophylaxis is an action taken to prevent or protect against a specified disease. Greek in origin, from the word “phylax”, meaning “to guard” and “watching.”
Low Risk Patients
Young healthy people do not need prophylaxis against
COVID-19. In young and healthy people, this infection causes mild
cold-like symptoms. It is advantageous for these patients to be exposed to COVID-19, build up their antibodies and have their immune system clear the virus. This will facilitate the development of herd immunity and help prevent future COVID-19 pandemics. However, if these patients desire prophylaxis against COVID-19, then they should take the protocol noted below.
Moderate-Risk Patients
Patients from this category are healthy but have high potential viral-load exposure. This
group includes medical personnel, caregivers of high-risk patients,
people who use public transportation, first responders and other
essential personnel who are crucial to the continued functioning of society. These patients should be encouraged to take prophylaxis against COVID-19 in accordance with the protocol noted below.
High-Risk Patients
Patients are considered high risk if they are over
the age of 60, or if they are younger than 60 but they have
comorbidities, that is, they have other health conditions that put them
at risk. These patients have between a 5 to 10 percent mortality rate if
they are infected with COVID-19. These patients should be strongly encouraged to take prophylaxis against COVID-19 in accordance with the protocol noted below.
Protocol for Low and Moderate Risk Patients:
Elemental Zinc 25 mg once a day[1]
Vitamin C 1000 mg once a day[2]
Quercetin 500 mg once a day
If Quercetin is unavailable, then use Epigallocatechin-gallate (EGCG) 400 mg once a day[3]
Protocol for High-Risk Patients:
Elemental Zinc 25 mg once a day
Hydroxychloroquine (HCQ[4]) 200 mg once a day for five days, then once a week
If HCQ is unavailable, then use the Protocol for Low and Moderate Risk Patients.”
[1]https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7365891/
[2]https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7318306/
[3]https://pubs.acs.org/doi/10.1021/jf5014633
[4]https://www.preprints.org/manuscript/202007.0025/v1
…………………………………….
Additional source, early outpatient treatment:
May 27, 2020, “Early
Outpatient Treatment of Symptomatic, High-Risk COVID-19 Patients That
Should Be Ramped Up Immediately as Key to the Pandemic Crisis,” Dr. Harvey A. Risch, American Journal of Epidemiology
…………………………………………..
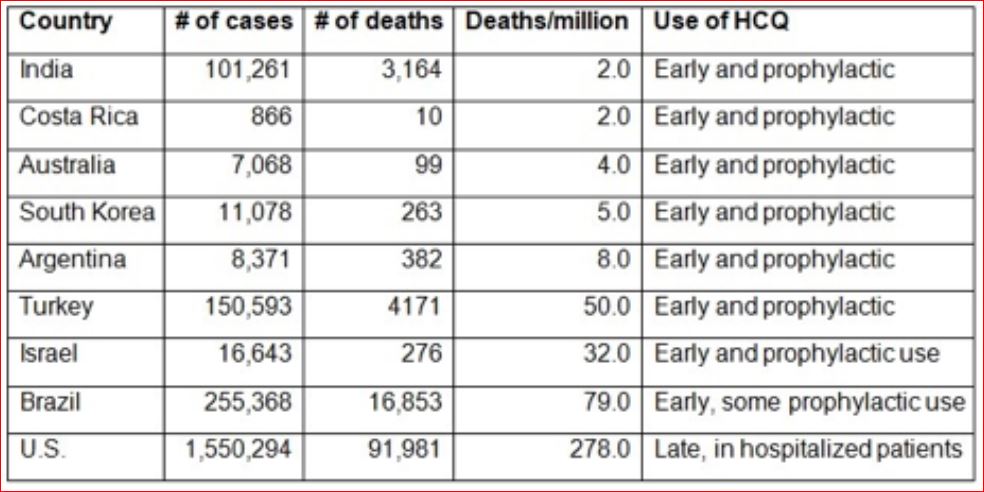
Added: Dramatically lower death rates in countries allowing early HCQ protocol and widespread prophylactic use:
May 29, 2020, “Break the FDA Barriers! Make Hydroxychloroquine Over-The-Counter,” Elizabeth Lee Vliet, MD, Preventive Medicine
A study by Dr. Harvey A. Risch, professor at Yale’s School of Public Health, “of hydroxychloroquine plus azithromycin in more than 300,000 older adults, just published May 27, 2020 said: “Evidence about use of hydroxychloroquine alone, or of hydroxychloroquine+azithromycin in inpatients, is irrelevant concerning efficacy of the pair in early high-risk outpatient disease. Five studies, including two controlled clinical trials, have demonstrated significant major outpatient treatment efficacy…These medications need to be widely available and promoted immediately for physicians.”
Early treatment with HCQ, and widespread prophylactic use, are the critical factors that led to the dramatically lower death rates in countries such as India (2/million), Australia (4/million), South Korea (5/million), Argentina (8/million) as of May 18.
By delaying HCQ use until people are already critically ill in the hospital, the US now has a markedly higher death rate from
COVID-19 (278/one million population as of May 18), even though we had
adequate hospital beds, ventilators and other equipment. Data by countries on May 18, 2020, which is updated daily, shows the stunning differences:
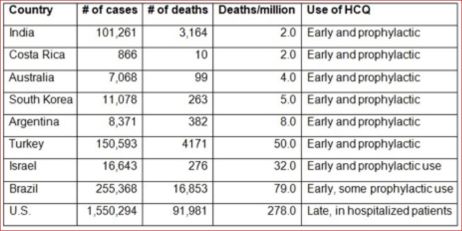
[Ed. note: I couldn’t find above chart or any mention of HCQ at the Worldometers link provided. The author may have used Worldometers numbers and added HCQ policy from other sources.]
………………………………………….
Added: HCQ protocol status by country:
11/14/20, “Early treatment with hydroxychloroquine: a country-based analysis,” hcqtrial.com…Twitter site, Covid Analysis
“Covid Analysis, August 5, 2020 (Version 35, November 14, 2020)“…[Covid Analysis twitter site]
…..
We are PhD researchers, scientists, people who hope to make a contribution, even if it is only very minor. You can find our research in journals like Science and Nature. For examples of why we can’t be more specific search for “raoult death threats” or “simone gold fired”. We
have little interest in adding to our publication lists, being in the
news, or being on TV (we have done all of these things before but feel
there are more important things in life now).
There is no need to. We provide organization and analysis, but all sources are public and you can easily verify everything.
For the country-based analysis, all data is public and the analysis is
simple to replicate. We also note that many equally qualified experts
report contradictory conclusions. If you don’t like our analysis, you can use our database to locate information you may have missed for your own research.
We have no funding, this is done in our spare time and we pay the web hosting fees personally (about $100 per month).”
“Results
Appendix 13. Country HCQ Status…
Australia, New Zealand, North Korea, Turkmenistan, Solomon Islands, Vanuata, Samoa, Kiribati, Federated States of Micronesia, Tonga, Marshall Islands, Palua, Tuvalu, Nauru
These countries were excluded because they have no or very little spread to date. They may be included in the future if they experience significant spread.
Bahrain – widespread early treatment (excluded due to young population)
Belarus – mixed use of early treatment with HCQ
Brazil – early HCQ treatment was adopted relatively late
Late and very mixed use, increasing over time.
Burkina Faso – widespread early treatment (excluded due to young population)
Cameroon – widespread early treatment (excluded due to young population)
.......
Canada – limited early treatment with HCQ
Chad – widespread early treatment (excluded due to young population)
Chile – mixed use of early treatment with HCQ
............
Costa Rica – widespread early treatment for high-risk patients for most of the outbreak. Used early based on recommendation from China 3/18.
............
Cuba – widespread early treatment for high-risk patients for most of the outbreak. Using to treat at an early stage.
Czech Republic – widespread early treatment (excluded due to early isolation)
Supported use since early March.
Djibouti – widespread early treatment (excluded due to small population)
...........
France – limited early treatment with HCQ
................
Germany – mixed use of early treatment with HCQ
Ghana – widespread early treatment (excluded due to young population)
Greece – widespread early treatment for high-risk patients for most of the outbreak
Guinea – widespread early treatment (excluded due to young population)
..........
India – widespread early treatment for high-risk patients for most of the outbreak
Indonesia – widespread early treatment (excluded due to early isolation)
.......
Ireland – limited early treatment with HCQ
Israel – mixed use of early treatment with HCQ
We initially
believed that Israel had widespread early use for the majority of the
outbreak, but we received reports that Israel’s use for early treatment has not be as widespread as believed.
Italy – early HCQ treatment was adopted relatively late
Malaysia – mixed use of early treatment with HCQ
Used early since January until about 6/22.
Mexico – limited early treatment with HCQ
...........
............
.......
Pakistan – mixed use of early treatment with HCQ
Obtained from India, later banned.
Panama – mixed use of early treatment with HCQ
Dropped usage at the end of May, started again in July
Peru – early HCQ treatment was adopted relatively late
.............
Portugal – mixed use of early treatment with HCQ
Qatar – widespread early treatment (excluded due to young population)
Senegal – widespread early treatment for high-risk patients for most of the outbreak
Used early. Prof. Raoult was born in Senegal.
.........
South Korea – widespread early treatment (excluded due to early isolation)
............
Spain – early HCQ treatment was adopted relatively late
.............
Sweden – limited early treatment with HCQ
Doctors instructed not to use.
.......
Switzerland – early HCQ treatment was adopted relatively late
Started using May 1.
Tunisia – mixed use of early treatment with HCQ
........
Turkey – widespread early treatment for high-risk patients for most of the outbreak
.......
........
......
......
Venezuela – widespread early treatment (excluded due to early isolation)
...............