
.
11/16/21, “Geert Vanden Bossche Was Right, The World’s Most Vaccinated Country Cancels Christmas Due to Massive Rise in COVID-19 Infections,” sundance
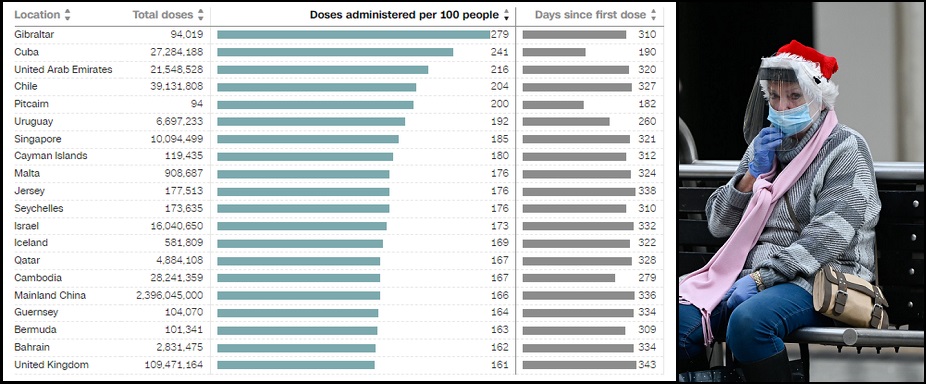
 “The most vaccinated population in the world exists on Gibraltar, a British commonwealth located at the southern end of Spain. The average number of vaccinations is 2.79 per person for all residents.
“The most vaccinated population in the world exists on Gibraltar, a British commonwealth located at the southern end of Spain. The average number of vaccinations is 2.79 per person for all residents.
However, even with that level of vaccination density, or perhaps –more likely– because of that level of vaccination density, the narrow peninsula is experiencing a massive rise in COVID-19 infections. As a result, the Gibraltar government announced today that all Christmas assemblies must be stopped, and citizens must re-evaluate their intent to gather in celebration of the birth of Jesus Christ.
UK News – “[…] In a statement released by the Gibraltar government, a spokesperson said: “Given the exponential rise in the number of cases, the Government, for example, intends to cancel a number of its own functions including official Christmas parties, official receptions and similar gatherings.
“The public, at this stage, are ultimately called upon to exercise their own judgement in this respect bearing in mind the current advice given….The Government strongly advises against any large informal social events, parties or receptions being held over at least the next four weeks while the vaccine booster programme is rolled out….Health Minister, the Hon Samantha Sacramento, described the increase in case numbers as “drastic”, encouraging people to come forward to receive their booster vaccine….
[In March [2021], Gibraltar became the first nation in the world to fully vaccinate its entire adult population [of approximately 34,000 people] against coronavirus.]…
“This consideration should include the number of persons, the setting whether indoor or outdoor, the degree of ventilation if indoor and whether those attending are vaccinated, elderly or vulnerable. “In the same way, as has happened in the past, this advice may change going forward.” (link)
This outcome in Gibraltar reminds me of the prior warning from Geert Vanden Bossche, a scientist and expert vaccine developer (Belgium) in September [2021].
When Vanden Bossche initially reviewed the high vaccination rates in Israel, Vanden Bossche warned the absence of a natural immunity population to fight the virus would lead to an uncontrollable spread of the virus in the vaccinated community. The higher the vaccination rates, the more serious the spread of the virus amid the population that only carries the immune system protection provided by the vaccine.
I encapsulated his outline here:
“The widespread vaccination rate is creating pressure on the virus to mutate into variants with higher levels of contagion. The unvaccinated group has been keeping the pressure down by defeating the virus and carrying natural immunity. However, as the unvaccinated population is increasingly made smaller, the pressure on the virus to mutate increases. Subsequently, these mutations stay at higher or more effective levels of infection.” [Image above of Gibraltar]
“Prompted to 17:09, Just Hit Play”
Posted, Sept. 2021, “Meeting of the COVID-19 Giants with Geert Vanden Bossche and Robert Malone MD"
0:00 Intro
05:45 mRNA Technology
11:50 Answer to Antivaxxers?
17:25 Are we where Geert expected?
20:45 COVID-19 in Israel
27:50 Geert explains selective immune pressure
48:00 Clarification of immune pressure by Robert
1:01:25 Explanation of ADE
1:11:40 How to communicate with Epidemiology leaders (Geert)
1:15:45 Explanation of Regulatory agencies (Robert)
1:30:15 Recommendation from Geert about strategies
1:40:45 Odd signals in the vaccine groups pointing to excess deaths
1:46:10 Explanation of infectious pressure graphs Time to listen and be open to change.
McMillan Research https://mcmillanresearch.com/”
……………………………………………
Extra: All of Gibraltar’s drinking water is desalinated seawater.
…………………………………………..
Added: “All prior vaccination campaigns [e.g., smallpox, polio, measles, yellow fever] involved live-attenuated virus.”
10/25/21, “Why can’t C-19 vaccine mandates be taken seriously?” GeertVanden Bossche.org
“Mass vaccination programs previously conducted to combat viral epidemics/pandemics (e.g., smallpox, polio, measles, yellow fever) have nothing in common with the ongoing mass vaccination campaigns today as those viruses are very different in terms of their pathogenesis, transmissibility, route of infection, potential reservoirs, predominant effector mechanisms involved in antiviral immunity, susceptibility of population segments, as well as with regard to the vaccines used (all prior vaccination campaigns involved live-attenuated virus).
In addition, vaccine efficacy as assessed during clinical trials is different from viral effectiveness, which reflects how well a vaccine performs in the field. Viral effectiveness, therefore, depends on the level of infectious pressure exerted by the viral population and the level of immune selection pressure exerted by the host population (among other factors). Those can be very different from the ones prevailing during clinical trials. This particularly applies when the vaccine is used in mass vaccination campaigns rolled out in the middle of a pandemic of more infectious variants. Because of large-scale pharmaceutical (e.g., mass vaccination) and nonpharmaceutical (e.g., infection-prevention measures) human interventions, significant changes in viral infectious pressure and population-level immune pressure can suddenly take place and dramatically accelerate or slow down the evolutionary dynamics of a pandemic, especially if more infectious variants are circulating.
Whereas the final target population should have the same profile as the one enrolled in the vaccine trials, current Covid-19 (C-19) vaccines are now administered to several segments of the population that have not been part of the pivotal clinical trials that enabled their authorization for emergency use (e.g., children, elderly, pregnant women, women of childbearing age, individuals who previously recovered from Covid-19 disease).
Furthermore, the follow-up of study participants in the clinical trials did not extend beyond 3 months as the WHO had declared the pandemic a health emergency of international concern. Short-term results from clinical vaccine trials that were conducted on a small subset of a specific target population during a short period of a pandemic caused by a specific SARS-CoV-2 lineage (most notably the original Wuhan strain) cannot even be considered informative for vaccine effectiveness of mass vaccination campaigns deployed globally across almost all population segments over a prolonged period of a pandemic trajectory involving several waves of infection caused by several different more infectious viral variants….
Stated more bluntly, short-term results from small-scale vaccine efficacy studies are anything but representative of the public health impact of these imperfect vaccines (*) when used in mass vaccination campaigns during a pandemic of more infectious variants.
This alone clearly illustrates that the use of current vaccines in the ongoing mass vaccination campaigns is purely experimental and empirical from a perspective of effectiveness on public health….
Furthermore, re-exposure to circulating viral variants in the presence of low affinity antibodies (**) could potentially provoke life-threatening antibody-dependent enhancement of C-19 disease (ADE). Clearly, results from clinical studies do not permit the drawing of any conclusions regarding the impact of viral exposure in the presence of low affinity antibodies….
It is important to note that previous efforts to develop a SARS-CoV-1 (***) vaccine had been abrogated due to the occurrence of ADE in preclinical models (7)….
Emerging data have shown that the S protein itself is a crucial element responsible for the vascular pathology of SARS-CoV-2 virus infection (8). Therefore, C-19 vaccines that induce human cells to produce the very same protein that is involved in viral pathogenicity should be carefully tested to make sure that such protein is not expressed systemically in the body after vaccination, or the effects of vaccination could result in a pathology similar to C-19 disease itself. However, data on the biodistribution in the human body of de novo synthesized S protein after vaccination are, for example, lacking and there were no pre-clinical animal studies done to evaluate this either. To this day, what tissues produce the S protein after vaccination with nucleic acid vaccines has not been conclusively elucidated, and concerning findings are emerging. The disproportionally high number of severe and common adverse events observed after administration of nucleic acid-based C-19 vaccines, such as deep-venous thrombosis, stroke, myocarditis, death, and others (9), suggests that the S protein can be expressed in a variety of tissues in the body, where it exerts pathogenic effects in subjects that experience adverse events. Many questions remain unanswered regarding the pathogenic mechanism underlying the observed vaccine-associated adverse events, while mass vaccination continues, and 16,310 deaths from C-19 vaccination have been reported as of October 1st, 2021, in the US alone (9).
Based on all the above, widespread deployment of current Covid-19 vaccines in large-scale vaccination campaigns should first and foremost be considered highly experimental and empirical in terms of the efficacy and safety (****) outcome as well as in terms of the impact on individual and public health. Because the experimental use of current Covid-19 vaccines raises serious concerns regarding their effectiveness and their potential to cause serious harm to both individuals and the public at large, one can only conclude that vaccination mandates are completely unethical.”
(*) ‘imperfect’ vaccine relates to a vaccine that has no viral transmission-blocking capacity
(**) Low affinity binding of anti-S antibodies may occur when titers of vaccinal antibodies against viral variants wane or as a result from asymptomatic infection of unvaccinated persons.
(***) SARS-CoV-1 is another beta-coronavirus; it emerged in 2003 (in Guangdong Province, China) and caused severe acute respiratory syndrome coronavirus (SARS-CoV).
(****) An extensive description of reported safety issues associated with one or more Covid-19 vaccines can be found at: https://docs.google.com/document/d/1AD0lL3Rm4lDExo4q7McBxeeHOqO8bCWWerlGu7YJubQ/edit
References
-
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5861807/pdf/khvi-14-03-1373228.pdf
-
https://journals.plos.org/plospathogens/article?id=10.1371/journal.ppat.1008857
-
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0250780
-
SARS-CoV-2 Spike Protein Impairs Endothelial Function via Downregulation of ACE 2 – PubMed (nih.gov)
-
VAERS Summary for COVID-19 Vaccines through 10/1/2021 – VAERS Analysis”
.....................
No comments:
Post a Comment